Monday, December 5, 2016
Thursday, November 3, 2016
Monday, October 10, 2016
Wednesday, October 5, 2016
Vestibular Symptoms
What are the symptoms of a vestibular disorder?
 The
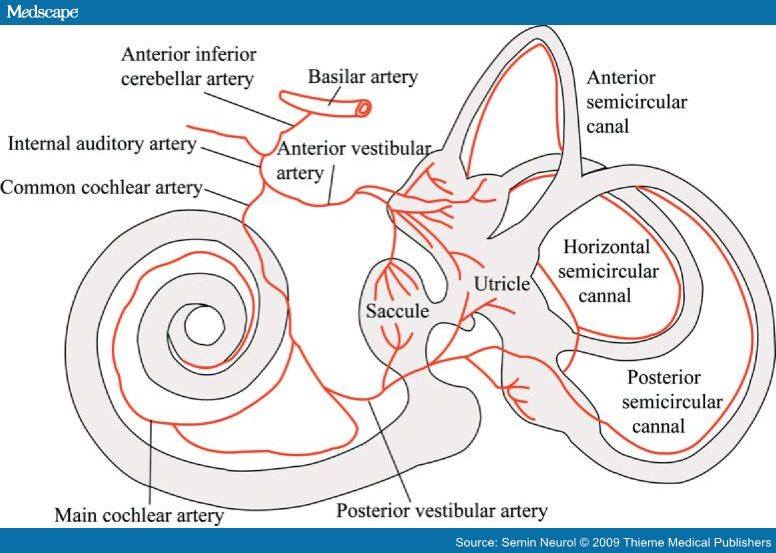
vestibular system includes the parts of the inner ear and brain that
help control balance and eye movements. If the system is damaged by
disease, aging, or injury, vestibular disorders can result, and are
often associated with one or more of these symptoms, among others:
The
vestibular system includes the parts of the inner ear and brain that
help control balance and eye movements. If the system is damaged by
disease, aging, or injury, vestibular disorders can result, and are
often associated with one or more of these symptoms, among others:- Vertigo and dizziness
- Imbalance and spatial disorientation
- Vision disturbance
- Hearing changes
- Cognitive and/or psychological changes
- Other symptoms
The type and severity of symptoms can vary considerably, and be frightening and difficult to describe. People affected by certain symptoms of vestibular disorders may be perceived as inattentive, lazy, overly anxious, or seeking attention. They may have trouble reading or doing simple arithmetic. Functioning in the workplace, going to school, performing routine daily tasks, or just getting out of bed in the morning may be difficult for some people.
Vertigo and dizziness
- Spinning or whirling sensation; an illusion of movement of self or the world (vertigo)
- Lightheaded, floating, or rocking sensation (dizziness)
- Sensation of being heavily weighted or pulled in one direction
Balance and spatial orientation
- Imbalance, stumbling, difficulty walking straight or turning a corner
- Clumsiness or difficulty with coordination
- Difficulty maintaining straight posture; tendency to look downward to confirm the location of the ground
- Head may be held in a tilted position
- Tendency to touch or hold onto something when standing, or to touch or hold the head while seated
- Sensitivity to changes in walking surfaces or footwear
- Muscle and joint pain (due to struggling with balance)
- Difficulty finding stability in crowds or in large open spaces
Vision
- Trouble focusing or tracking objects with the eyes; objects or words on a page seem to jump, bounce, float, or blur or may appear doubled
- Discomfort from busy visual environments such as traffic, crowds, stores, and patterns
- Sensitivity to light, glare, and moving or flickering lights; fluorescent lights may be especially troublesome
- Sensitivity to certain types of computer monitors and digital televisions
- Tendency to focus on nearby objects; increased discomfort when focusing at a distance
- Increased night blindness; difficulty walking in the dark
- Poor depth perception
Hearing changes
- Hearing loss; distorted or fluctuating hearing
- Tinnitus (ringing, roaring, buzzing, whooshing, or other noises in the ear)
- Sensitivity to loud noises or environments
- Sudden loud sounds may increase symptoms of vertigo, dizziness, or imbalance
Cognitive
- Difficulty concentrating and paying attention; easily distracted
- Forgetfulness and short-term memory lapses
- Confusion, disorientation, difficulty comprehending directions or instructions
- Difficulty following speakers in conversations, meetings, etc., especially when there is background noise or movement
- Mental and/or physical fatigue out of proportion to activity
Psychological
- Loss of self-reliance, self-confidence, self-esteem
- Anxiety, panic, social isolation
- Depression
Other
- Nausea or vomiting
- "Hangover" or "seasick" feeling in the head
- Motion sickness
- Sensation of fullness in the ears
- Headaches
- Slurred speech
- Sensitivity to pressure or temperature changes and wind currents
- Pain, pressure, or other symptoms with certain dietary changes (e.g., high sodium)
Sunday, September 11, 2016
Monday, August 29, 2016
Friday, August 19, 2016
Wednesday, August 10, 2016
Monday, August 1, 2016
Thursday, July 21, 2016
Wednesday, June 29, 2016
Tuesday, June 28, 2016
Wednesday, June 22, 2016
Wednesday, June 15, 2016
Tuesday, June 7, 2016
Monday, May 30, 2016
Saturday, May 28, 2016
Sunday, May 22, 2016
Saturday, May 21, 2016
Wednesday, May 18, 2016
Friday, May 13, 2016
Behind the Brand with Dr. Bogan
Friday, May 6, 2016
Saturday, April 30, 2016
Parasomnia
http://blog.soundsleephealth.com/parasomnia-definition-things-that-go-bump-in-the-night-sleepwalking-sexsomnia
Thursday, April 28, 2016
Drunk
http://www.theguardian.com/commentisfree/2016/apr/28/sleep-study-workers-deprived-same-as-vodka-shots
Monday, April 25, 2016
Petition to add Narcolepsy to SSA's list of disabling illnesses
Please sign the
petition asking Congress to include Narcolepsy as a disabling condition
in the Social Security Administration's "Blue Book".
Did
you know that narcolepsy is not considered a disabling condition by the
Social Security Adminstration? It's true. Because of that, the
application of a narcoleptic for Social Security Disability Benefits
(SSDI) will almost always be denied, requiring often two appeals before
the application finally goes before an Executive Law Judge at the State
level. It is incredibly difficult for a narcoleptic to get SSDI,
normally taking an average of THREE YEARS to go through the entire
process.
A
friend of ours, Sharon Denise Remo, has put up a petition on the US
Congress' web site asking that narcolepsy be added to SSA's list of
disabling illnesses, something that would tremendously speed up the
process of getting SSDI. Please sign the petition. You can find it
at:
We will all be very grateful to you. Thanks!
Monday, April 11, 2016
Monday, April 4, 2016
Saturday, April 2, 2016
Monday, March 28, 2016
Friday, March 25, 2016
Snooze alarm
My great uncle, Collins Mason, and Carl A. Imhoff invented this!
https://patents.google.com/patent/US2636337A/en?q=collins&q=mason+alarm
https://patents.google.com/patent/US2636337A/en?q=collins&q=mason+alarm
Thursday, March 3, 2016
Lack of sleep
http://articles.mercola.com/sites/articles/archive/2016/03/03/sleep-deprivation-effects.aspx?e_cid=20160303Z1_DNL_art_1&utm_source=dnl&utm_medium=email&utm_content=art1&utm_campaign=20160303Z1&et_cid=DM99252&et_rid=1384317314
Monday, February 29, 2016
Form of baclofen works better at treating narcolepsy
Form of baclofen works better at treating narcolepsy: Neuroscientists at SRI International have found that a form of baclofen, a drug used to treat muscle spasticity, works better at treating narcolepsy than the best drug currently available when tested in mice.
Friday, February 19, 2016
Experiencing Narcolepsy
PWNs experience NC in many different ways with various symptoms. I have been to many Dr appts where I was asleep most of the time I was there. It might have looked like I was drunk because I was staggering around, slurring my speech and having problems concentrating. It's especially worse. Now I make sure I take something warm because cold temperatures will make me go to sleep. Warm temperatures keep me awake. Sometimes I will open my bedroom window when it's 30 degrees outside because I'm too warm.
What do I do? I have to record my appt before my appt - describe my symptoms, what I need help with, etc - because it might not be comprehended from my speech while I'm there. You might say - take an advocate. That works well if the person I take is familiar with my condition. The best advocate I had has Hoshimotos. She knows what it's like to not be able to think, have memory problems and being dead tired and sleepy. She could understand my problems
Below is how another PWN experiences narcolepsy:
Ok so when I have one of my worst days these are things I experience I want to know what some of you go thru I get everybody is different in every case but a lot of us feel that with narcolepsy the surface is merely being scratched so I'm gonna post a normal daily list also
On a bad day:
Irritability, struggle with using my hands to do things, I struggle speaking, i.e.. shuddering finding the words to talk pauses in speaking, losing my thoughts,
Memory, my legs don't work, extreme weakness, muscles move like jello
I get that dead numb empty feeling in my parts, almost collapsing I feel as if I'm shaking though I'm perfectly still, I feel extremely exhausted more then normal, to weak to move on my own, emotional, headaches, dizzy, blurred vision, hotter then usually to where I sit in a cold shower or open the Windows, "it's winter in Wisconsin pretty cold teens and lower"
Normal day: normal tired, ok strength, typically warm body temperature, tolerable RLS, IBS, numbness due to taking glutamate along with slower speech & motor skills, always losing things,forgetting stuff constantly,
Uncontrolled muscle twitching, and dipping when walking or standing I use a cane so I usually don't fall
"A week ago I was with my boyfriend he started to slow.dance with me n my legs kept dipping as I made my way to the couch got really tired I felt as if checked out for about 5 or 10 mins and then I was fine" I think it was an attack but I'm really not sure as it doesn't happen much I just get weak knees n dip a few times and that was the worst I remember???
All I can remember right now as yesterday was a bad day but I'd like to hear what some of you others go through as this is still kind of new for me
What do I do? I have to record my appt before my appt - describe my symptoms, what I need help with, etc - because it might not be comprehended from my speech while I'm there. You might say - take an advocate. That works well if the person I take is familiar with my condition. The best advocate I had has Hoshimotos. She knows what it's like to not be able to think, have memory problems and being dead tired and sleepy. She could understand my problems
Below is how another PWN experiences narcolepsy:
Ok so when I have one of my worst days these are things I experience I want to know what some of you go thru I get everybody is different in every case but a lot of us feel that with narcolepsy the surface is merely being scratched so I'm gonna post a normal daily list also
On a bad day:
Irritability, struggle with using my hands to do things, I struggle speaking, i.e.. shuddering finding the words to talk pauses in speaking, losing my thoughts,
Memory, my legs don't work, extreme weakness, muscles move like jello
I get that dead numb empty feeling in my parts, almost collapsing I feel as if I'm shaking though I'm perfectly still, I feel extremely exhausted more then normal, to weak to move on my own, emotional, headaches, dizzy, blurred vision, hotter then usually to where I sit in a cold shower or open the Windows, "it's winter in Wisconsin pretty cold teens and lower"
Normal day: normal tired, ok strength, typically warm body temperature, tolerable RLS, IBS, numbness due to taking glutamate along with slower speech & motor skills, always losing things,forgetting stuff constantly,
Uncontrolled muscle twitching, and dipping when walking or standing I use a cane so I usually don't fall
"A week ago I was with my boyfriend he started to slow.dance with me n my legs kept dipping as I made my way to the couch got really tired I felt as if checked out for about 5 or 10 mins and then I was fine" I think it was an attack but I'm really not sure as it doesn't happen much I just get weak knees n dip a few times and that was the worst I remember???
All I can remember right now as yesterday was a bad day but I'd like to hear what some of you others go through as this is still kind of new for me
Communicating with your doctor about Narcolepsy
The other day, I posted a question on Facebook: If you wanted to find out if a doctor knew something about
narcolepsy (not a sleep doctor but a regular doctor), what questions would you ask him/her?
One of my friends gave a really good reply. I have posted it below.
I wouldn't even bother asking a doc who
is not a sleep doc, and even then that gets tricky to do without
offending them.
My PCP is an internist with a specialty in geriatrics. He freely admits I know more about N than he ever will and when he has a new doc in his office on an internship, he has me educate them on N.
My PCP is an internist with a specialty in geriatrics. He freely admits I know more about N than he ever will and when he has a new doc in his office on an internship, he has me educate them on N.
Perhaps, Anne,
a better way might be to say, "I realize that N is barely
covered in medical school and if you went to med school more than 15
years ago they still thought it was a psychological problem. However,
it would be very helpful in establishing our doctor-patient
relationship if you'd agree to two things: 1. Be honest with me about
what you do or don't know about N, and 2. Accept that I may know more
than you on that subject and be willing to listen to me.
I think also, and I've done this, make
it mandatory that your PCP and your sleep doc share notes after every
visit to one or the other. As well, you might suggest to the primary
that he talk to the sleep doc and get confirmation that you know what
you're talking about. Gives you much more credibility. Alternatively,
you might try getting a letter of introduction from your sleep doc
that states specifically that you are a well educated patient and
what you say is well informed and should be taken seriously. Come to
think of it, that might even be the best approach.
Further, it *IS* important to remember
that docs have worked very hard to get to be where they are, and even
if some of them are arrogant bastards we still do need to recognize
that they are thinking that it's pretty chutzpadig of you to presume
to tell them they don't know what they're talking about. And never
say "I saw this thing on the net that said...". Only say,
"I read an article (on PubMed but don't include this) in such
and such a journal that said..." Citing the journal is very
important to establishing your credibillity. Print it out and bring
it with you. I've done that. It takes all the wind out of their
sails.
Monday, February 15, 2016
Thursday, February 11, 2016
To the Doctors of Chronic Illness Patients
Dear Doctor,
Unless you keep up with ALL the new information on narcolepsy or you are my sleep doctor, I know more about my condition than you do. What it affects, and what happens when you get it wrong. When I write in very bold letters that my TSH is best at 2, believe me! When I tell you I get cataplexy when it gets over 3, believe me! When you see me walking weirdly, sort of herky-jerky, believe me when I tell you I have a lot of pain. Do you think you can believe me?
Click the post title to link to the article on themighty.com.
Unless you keep up with ALL the new information on narcolepsy or you are my sleep doctor, I know more about my condition than you do. What it affects, and what happens when you get it wrong. When I write in very bold letters that my TSH is best at 2, believe me! When I tell you I get cataplexy when it gets over 3, believe me! When you see me walking weirdly, sort of herky-jerky, believe me when I tell you I have a lot of pain. Do you think you can believe me?
Click the post title to link to the article on themighty.com.
No Thirst
Many narcoleptics have no thirst mechanism. I'm never thirsty even though my mouth may be parched. I copied this from a post by Moshe Turner.
Dynorphin is co-localised on orexin neurons (but not exclusively). With the loss of orexin neurons, dynorphin levels drop. Vasopressin, which regulates vascular tone, responds to dehydration by trying to narrow blood vessels, which raises blood pressure. This process is modulated by dynorphin such that even as vasopressin neurons are receiving spiking electrical signals telling them to release more neurotransmitter, dynorphin is saying no, chill out on the vasopressin. Because lower vasopressin levels cause a person to get thirsty, the person knows to drink. Without adequate dynorphin, vasopressin levels rise and the thirst response is repressed; PWN don't get thirsty when we get dehydrated; in other words we "forget" to drink, which leads to various health problems.
In other words, drink more water!
Dynorphin is co-localised on orexin neurons (but not exclusively). With the loss of orexin neurons, dynorphin levels drop. Vasopressin, which regulates vascular tone, responds to dehydration by trying to narrow blood vessels, which raises blood pressure. This process is modulated by dynorphin such that even as vasopressin neurons are receiving spiking electrical signals telling them to release more neurotransmitter, dynorphin is saying no, chill out on the vasopressin. Because lower vasopressin levels cause a person to get thirsty, the person knows to drink. Without adequate dynorphin, vasopressin levels rise and the thirst response is repressed; PWN don't get thirsty when we get dehydrated; in other words we "forget" to drink, which leads to various health problems.
In other words, drink more water!
Orexin's Many Roles
If you have narcolepsy, orexin cells are destroyed in the hypothalamus. Orexin seems to play a role in a large number of problems in many illnesses.
Click the post title to go to the article on http://www.ncbi.nlm.nih.gov.
Click the post title to go to the article on http://www.ncbi.nlm.nih.gov.
Wednesday, February 10, 2016
The art of asking the right questions.
Unfortunately the art of asking questions seems to be lost . There's too much assuming . How hard is it to just ask . I've gotten very thin alot of PWN are thin . The med takes away your appetite . The other assumption because I'm sleepy and fatigued that I don't get any exercise . I'm constantly moving it keeps me awake. I go and down stairs all day. That I don't hurt all over just so used to it forget to mention this. I don't understand how anyone could miss . If they see me floundering trying to keep myself upright when my muscles feel weak . Here's an area for an assumption . Wouldn't you think they would assume with all those movements I just might have alot of pain
Thursday, February 4, 2016
Physicians who profess to know something about NC.
This is a very serious problem.If your other physicians say they know about NC you can't be sure. These are physicians other than your sleep Dr. It makes no difference if they say they treat someone with NC . If they're a neurologist and have a few patients with NC watch out.
They're judging your NC by their other patients with NC. Everyone's NC is so different why oh why don't these other Drs know that? What would have happened to me if I hadn't been diagnosed with NC is frightening . I never realized how lucky I was to have gone to Dr. G in 2001.
Keeping up with and correcting Dr. mistakes is disheartening. Today I just found out I had childhood ADD without hyperactivity. Since my Dad was a surgeon surprised he missed that . This particular Dr knew I had NC but he obviously didn't know enough. No telling what he thought when I was having cataplexy during one of my office visits. He wanted to know if they needed to call an ambulance. Why oh why can't they even get my med information right . Giving them my medical information page just doesn't seem to work .
Most Drs don't have time to keep up with current information on NC . It's not a just a minor sleep disorder. It's a brain disease.
They're judging your NC by their other patients with NC. Everyone's NC is so different why oh why don't these other Drs know that? What would have happened to me if I hadn't been diagnosed with NC is frightening . I never realized how lucky I was to have gone to Dr. G in 2001.
Keeping up with and correcting Dr. mistakes is disheartening. Today I just found out I had childhood ADD without hyperactivity. Since my Dad was a surgeon surprised he missed that . This particular Dr knew I had NC but he obviously didn't know enough. No telling what he thought when I was having cataplexy during one of my office visits. He wanted to know if they needed to call an ambulance. Why oh why can't they even get my med information right . Giving them my medical information page just doesn't seem to work .
Most Drs don't have time to keep up with current information on NC . It's not a just a minor sleep disorder. It's a brain disease.
Sunday, January 10, 2016
If this is the first time you've been to my blog go to the December 23 the second posting or maybe it's Dec 27 . I didn't write the second posting .I copied it from a facebook support group page . It might explain one of my problems. If you're sleep deprived your memory and thinking are impaired. Now it's not as bad as it used to be since I take supplements that help with those problems. If you see me I might look drunk, talk weird, look as if I'm in a trance,or I might fall down all of a sudden. I take 60mg of generic adderal. That does not always keep me awake nor does it help with the constant fatigue. Sometime it makes me very irritating to be around. It's irritating to me too .I had a MSLT test to confirm my diagnosis. No One is going to take you seriously even if you're falling down with cataplexy. Most of your friends won't get it or understand . Fortunately my family understands. I consider close friends as a member of my family. The only Dr that understands all of my symptoms is my sleep Dr. One particular neurologist who must have had only one patient with NC didn't even understand my cataplexy or that I could take such a strong dose of a med and not have a hard time falling asleep at night. Most PWN are in and out of rem so many have insomnia. They might wake up many times a night. Luckily I have an understanding family medicine Dr.
I have to explain my weirdness that's it's normal for PWN so if I see a new Dr they don't flip out or come up with another diagnosis like weird talking syndrome. It takes alot of work but you have to keep track of your medical problems, all your labs results past results etc. I once went to this place I call the palace of malice . I had called asked about getting my records and how hard it was to find anyone that knew anything about N. Well we have one such person in our palace. The palace was easier to drive to than other places just took longer to get there. I had stopped driving on highways. Did this person know anything about NC ? No, she knew very little . I wasn't going there to be treated for my NC. They should be aware of some of my symptoms. Unfortunately the person didn't pay any attention to my boldly written My TSH is best at 2.00 if it goes up let me know . It kelp going up and up to 4.39 . That's when I started having cataplexy all the time. I found this put at another appt . Even the endo I went to ignored my paper. By then I was falling asleep at his appointment . The person who thought she was a health provider was very fluent in sounds good so I'll add that on her report
I have to explain my weirdness that's it's normal for PWN so if I see a new Dr they don't flip out or come up with another diagnosis like weird talking syndrome. It takes alot of work but you have to keep track of your medical problems, all your labs results past results etc. I once went to this place I call the palace of malice . I had called asked about getting my records and how hard it was to find anyone that knew anything about N. Well we have one such person in our palace. The palace was easier to drive to than other places just took longer to get there. I had stopped driving on highways. Did this person know anything about NC ? No, she knew very little . I wasn't going there to be treated for my NC. They should be aware of some of my symptoms. Unfortunately the person didn't pay any attention to my boldly written My TSH is best at 2.00 if it goes up let me know . It kelp going up and up to 4.39 . That's when I started having cataplexy all the time. I found this put at another appt . Even the endo I went to ignored my paper. By then I was falling asleep at his appointment . The person who thought she was a health provider was very fluent in sounds good so I'll add that on her report
Subscribe to:
Posts (Atom)